CMS Adds ICD-10-PCS Root Operation, Modifies Others in 2017 Update
CMS recently released the 2017 ICD-10-PCS code updates and guidelines, which include changes to certain root operations. Of the updates, the most notable modifications are the addition of root operation Perfusion, and edits to the current definitions of Control and Creation.
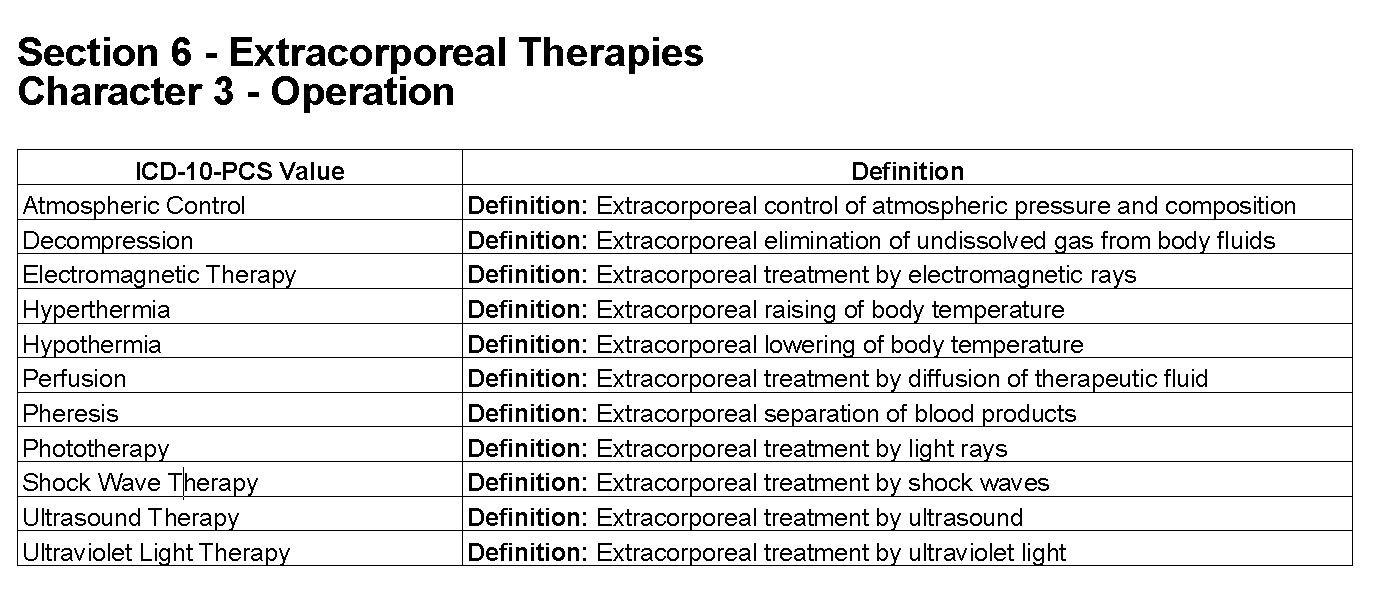
Root operation Perfusion has been added to the Extracorporeal Therapies section. CMS defines Perfusion as an “extracorporeal treatment by diffusion of therapeutic fluid.” The full Extracorporeal Therapies definitions’ chart can be found in CMS’ ICD-10 Procedure Coding System 2017 Tables and Index.
{kind=link}
CMS now defines the root operation Control as stopping, or attempting to stop, postprocedural or other acute bleeding. “Other acute bleeding” is the new addition to the definition.
“If an attempt to stop postprocedural or other acute bleeding is initially unsuccessful, and to stop the bleeding requires performing any of the definitive root operations Bypass, Detachment, Excision, Extraction, Reposition, Replacement, or Resection, then that root operation is coded instead of Control,” said CMS.
The root operation Creation was defined in the 2014 ICD-10-PCS Reference Manual as, “making a new genital structure that does not physically take the place of a body part.”
CMS now defines Creation as “putting in or on biological or synthetic material to form a new body
part that to the extent possible replicates the anatomic structure or function of an absent body part.” This has changed the focus of this root operation to other body systems, whereas before, Creation focused on sex-change procedures.
Also updated by CMS is Excision for grafts. “If an autograft is obtained from a different procedure site in order to complete the objective of the procedure, a separate procedure is coded,” said CMS.
An example of this, CMS said, is coding a coronary bypass with excision of a saphenous vein graft. Excision of the saphenous vein would be coded separately.
“These guidelines have been developed to assist both the healthcare provider and the coder in identifying those procedures that are to be reported,” said CMS. “The importance of consistent, complete documentation in the medical record cannot be overemphasized. Without such documentation accurate coding cannot be achieved.”
All changes have been approved by the Cooperating Parties (CMS, the American Hospital Association, AHIMA, and the National Center for Health Statistics) and will be effective October 1, 2016.